


Innovation at University Hospitals Leads to Safer Same Day Procedure for Left Atrial Appendage Patients
October 25, 2020
Conscious sedation approach uses cardiac CTA for pre-procedure planning and intracardiac echo during the procedure
Innovations in Cardiovascular Medicine & Surgery | Fall 2020
 Steven Filby, MD
Steven Filby, MDThe clinical expertise gained from innovations in transcatheter aortic valve replacement (TAVR) and the challenges of the COVID-19 era have yielded an unexpected benefit for patients undergoing a procedure to occlude a left atrial appendage (LAA) at University Hospitals Harrington Heart & Vascular Institute, based at University Hospitals Cleveland Medical Center.
Instead of relying on transesophageal echocardiogram (TEE) guidance, the UH team now performs the LAA occluder procedure using cardiac CTA for pre-procedure planning and intracardiac echo during the procedure – an innovation that allows for the procedure to be safer, more efficient and performed with conscious sedation. Many patients go home the same day. From 2017 to 2019, the success rate was 99.1 percent. For 2020, it’s 100 percent.
“This grew out of our experience with other structural technologies, specifically TAVR,” says UH interventional cardiologist Steven Filby, MD. “We understood that using CTA imaging for that technology resulted in better outcomes. We just bridged this over for left atrial appendage. We gain important digital image information in terms of planning and puncturing the septum and then choosing the best course for device delivery.”
Safety precautions during the COVID-19 pandemic have also played a role in this innovation, Dr. Filby says, who is also Assistant Professor of Medicine at Case Western Reserve University School of Medicine.
“Under COVID precautions, no longer are physicians that inclined to do TEE,” he says. “When you do TEE, there's a possibility for microparticulate aerosolization of infectious material. Not only that, but we've come to understand that the placement of the TEE probe can lead to esophageal erosions -- a microtraumatic injury to the esophagus. So it’s not a benign procedure.”
Plus, Dr. Filby says, cardiac CTA has clear advantages of its own for LAA procedures.
The goal, as always, is making those incremental improvements that make a measurable difference in outcomes and patient safety.
“The importance of doing cardiac CT imaging for pre-procedural planning is that there is much better definition and image information about the appendage,” he says. “It’s a structure that varies tremendously from one individual to the next and can be very irregular in its shape. The appendage from one person to the next is as unique as a thumbprint. When traditional imaging using TEE is used, you don't necessarily get all the dimensions or the accurate dimensions of the appendage to determine the best size device. Also, with cardiac CTA, we're able to really take a really close look of the anatomy of the septum and puncture the septum at the best trajectory to deliver the catheter across the septum after that puncture so as to reach the left atrial appendage.”
Most patients undergoing the LAA procedure at UH complete the procedure in a single day, with 70 percent not requiring an overnight stay. Everything takes place in the Center for Advanced Heart & Vascular Care at UH Cleveland Medical Center, one of the first cardiovascular centers in the world to co-locate an MRI, CT and robotically operated cardiac catheterization laboratory with surgical capabilities in the same suite.
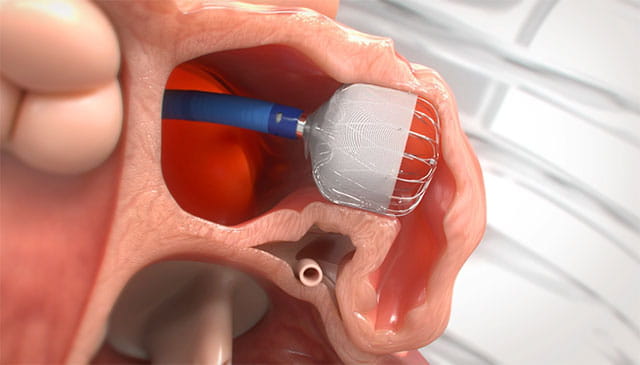 Schematic of WATCHMAN FLX device used in LAA procedures. Image courtesy of Boston Scientific.
Schematic of WATCHMAN FLX device used in LAA procedures. Image courtesy of Boston Scientific.“The cardiac CT scanner is right next to our hybrid cath lab in the same suite,” Dr. Filby says. “Literally you can see from one room to the next, so they get their cardiac CTA and then they get on the table for the procedure. It's one big day. This is especially helpful for those patients who live a distance away.”
Dr. Filby says the team at UH Harrington Heart & Vascular Institute is continuing to innovate in the LAA procedure, taking full advantage of the capabilities of the Center for Advanced Heart & Vascular Care.
“We're fusing the cardiac CTA and overlaying those images in real time with the fluoroscopy images,” Dr. Filby says. “We're literally opening up the CT scan, going into the chest, identifying the heart, identifying the left atrial appendage, and drawing it out, drawing out the appendage, drawing out the inner atrial septum. Then we take that image and we overlie on the patient who assumes a similar position on the table. We match up the rib structures, the bony structures, the sternum, the vertebral bodies. We match up the things that we can see so that those soft tissue structures that we have highlighted digitally can be represented upon the patient’s real time fluoroscopic image. When we step on the pedal, we see that image in real time of the drawing. So we know exactly where to put our catheter. It gives us yet another dimension, another image dimension to work with to make the procedure more efficient.”
The goal, as always, is making those incremental improvements that make a measurable difference in outcomes and patient safety.
“Our approach, with the combination of cardiac CTA and intracardiac echo, has led to a more efficient procedure and less potential injury to the patient, so it’s a safer procedure,” Dr. Filby says. “It’s also then a procedure from which the patient can more easily recover, which has led to a same-day discharge strategy.”
For more information about the UH approach to LAA or to refer a patient, please call 216-844-3800.