


Digital Tomosynthesis Enhances Care in Patients with Emphysema
June 27, 2023
Benefits include less radiation and financial savings
Innovations in Pulmonology & Sleep Medicine | Summer 2023
Bronchoscopic Lung Volume Reduction (BLVR) is a minimally invasive procedure that can help some patients with advanced emphysema breathe more comfortably. One-way valves in the airways prevent air from entering damaged portions of the lungs, while still allowing the evacuation of trapped air and secretions.
In carefully selected patients, BLVR has been shown to be helpful. However, about one-third of these patients are at risk of developing a pneumothorax, which has significant clinical implications. Because of that, timely detection is critical.
“Digital tomosynthesis (DTS) is one of the newer imaging modalities,” says Sameer Avasarala, MD, attending physician in the Division of Pulmonary, Critical Care and Sleep Medicine at University Hospitals Cleveland Medical Center. “It’s a form of digital radiography that has some of the benefits of chest CTs, but with additional advantages. In the pulmonology space, DTS can help clinicians detect complications following BLVR.”
 Sameer Avasarala, MD
Sameer Avasarala, MDDTS uses an X-ray tube and flat panel screen. As a computer-controlled crane tilts the X-ray tube at multiple angles, it moves over the target area in a linear path. Reconstruction algorithms allow the reader to scroll through the images in different planes.
“This technology helps us pick up things that we may not see in a standard chest radiography,” Dr. Avasarala says. “Chest radiography, or plain X-rays, are the quickest way to detect a pneumothorax or other abnormalities, but sometimes a CT scan is also needed. DTS closes that gap. It’s also roughly half the cost of a standard chest CT, and patients receive about 90 percent less radiation.”
 Robert Gilkeson, MD
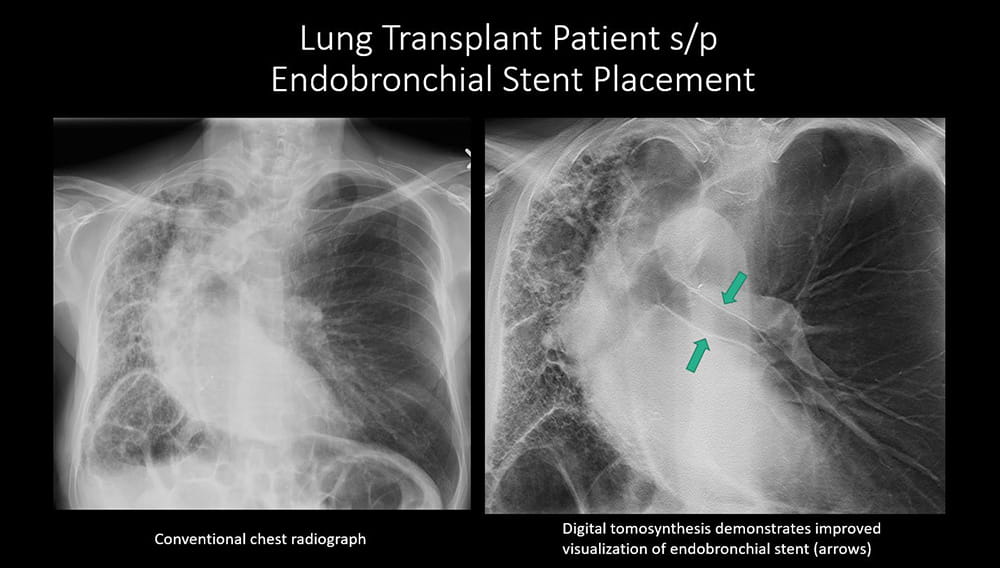
Robert Gilkeson, MDRobert Gilkeson, MD, Vice Chairman of Research at University Hospitals Cleveland Medical Center, says UH originally used DTS to improve detection of COVID-19 and has now expanded the tool to further improve pulmonary interventions, including lung transplantation, endobronchial valve therapy, tracheobronchial stent placement and pneumothorax detection.
DTS in Clinical Practice
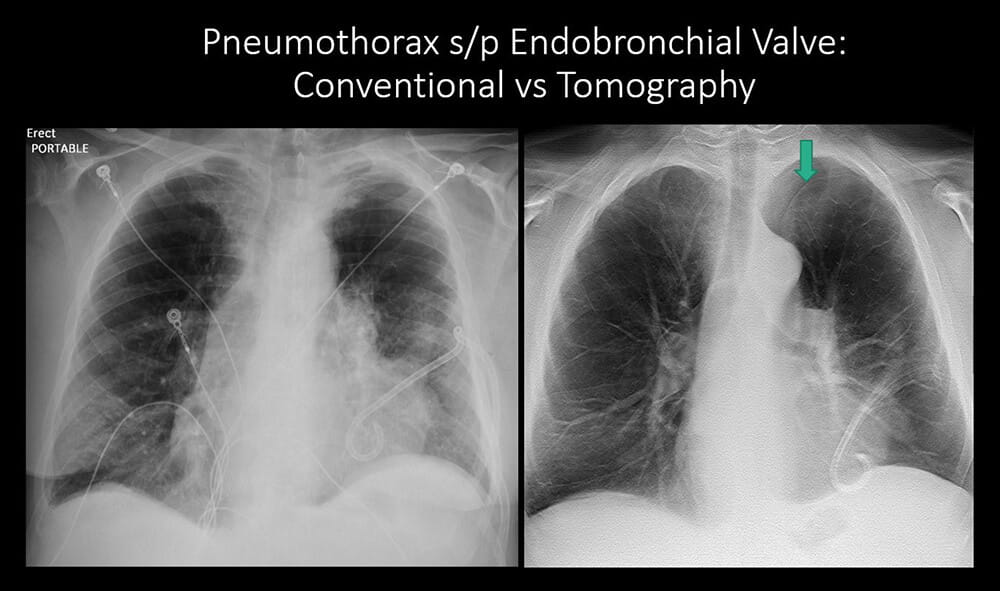
Drs. Avasarala and Gilkeson, with their colleague Benjamin Young, MD, director of bronchoscopy in the Division of Pulmonary, Critical Care and Sleep Medicine at University Hospitals Cleveland Medical Center, recently published a DTS case study in the American Journal of Respiratory and Critical Care Medicine. A patient with severe emphysema had six endobronchial valves placed. Following BLVR, she developed a pneumothorax on the day of the procedure. This was managed with a chest tube, which was removed four days later. A plain chest radiograph performed after the chest tube was removed failed to show a left apical pneumothorax that was only detected on the DTS image.
“This is critically important,” says Dr. Avasarala. “We don’t want to send patients home with a finding like this; it needs additional work up. This is a great example of a technology application that uses much less radiation than a CT scan and is more fiscally responsible.”
Unique Interdisciplinary Collaboration
“From an institutional standpoint, UH Cleveland Medical Center is a place that has both the DTS technology and expertise all in a one-stop shop,” says Dr. Avasarala. “This allows us to use imaging to detect chest complications or findings on patients’ chests that are not picked up on X-rays. Patients get better care and may avoid CT scans with their additional costs and radiation.
“This is another great example of collaboration between interventional pulmonology and thoracic radiology. It’s remarkable to see this type of collaboration between two specialties that depend on technological advancements and how one just makes the other better.”
For more information about DTS, contact Dr. Gilkeson at 216-844-1700.
Contributing Experts:
Sameer Avasarala, MD
Attending Physician
Division of Pulmonary, Critical Care and Sleep Medicine
University Hospitals Cleveland Medical Center
Assistant Professor
Case Western Reserve University School of Medicine
Robert Gilkeson, MD
Vice Chairman, Research
University Hospitals Cleveland Medical Center
Professor
Case Western Reserve University School of Medicine