


Standardizing Care for Pancreatic Cysts
February 10, 2019
New algorithm brings consistency to evaluation, surveillance and treatment, so patients ‘don’t get lost in follow-up’
Innovations in Digestive Health - Winter 2019
“Pancreatic cysts are a clinical conundrum for pancreatologists,” says Jordan Winter, MD, Chief of Surgical Oncology, University Hospitals Cleveland Medical Center, and Associate Professor of Surgery, Case Western Reserve University School of Medicine. “Some are concerning, some present a very low cancer risk and many fall in the middle. High-risk cysts aren't always obvious.”
 Jordan Winter, MD
Jordan Winter, MDPancreatic cyst treatment varies widely as the cysts themselves. Low-risk cysts require a “watch and wait” approach, while some high-risk cysts necessitate open surgery. Some cysts with malignant potential rarely progress to cancer. In that case, should the doctor recommend surgery or surveillance?
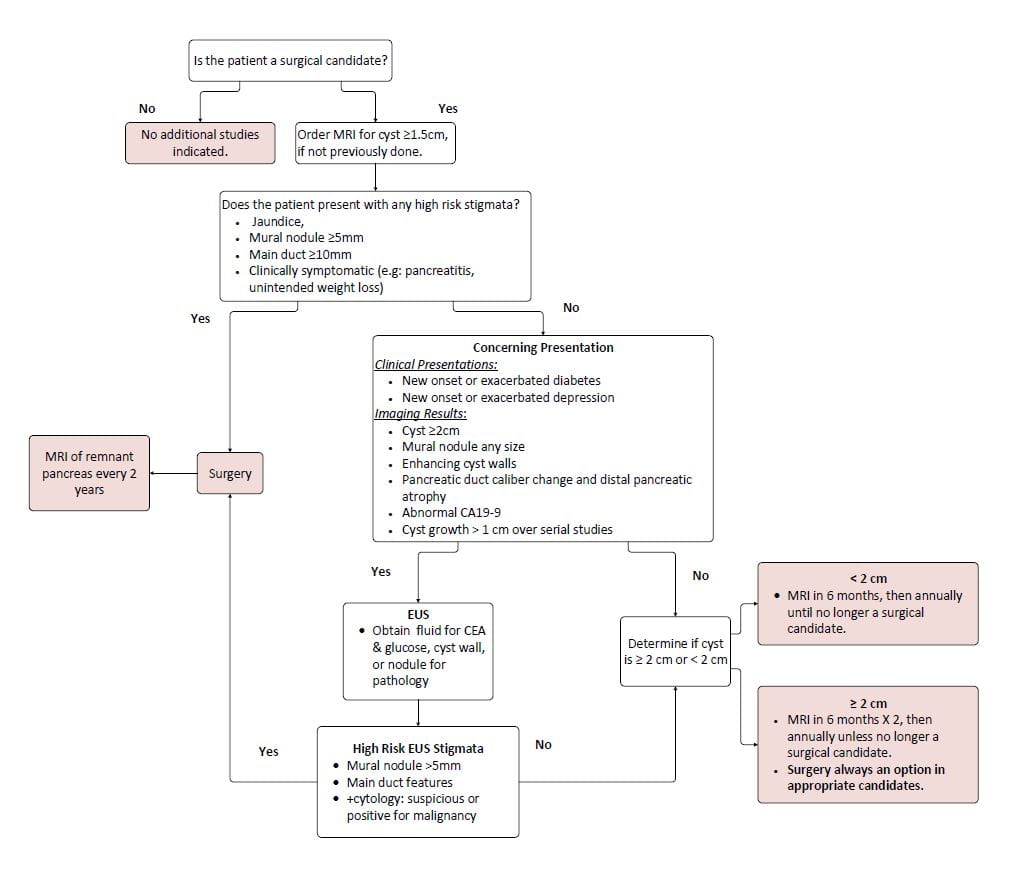
To help pancreatologists determine the most appropriate treatment, Dr. Winter and his UH Digestive Health Institute colleagues developed a “pancreatic cyst evaluation, surveillance and treatment algorithm.” The algorithm aims to bring consistency to a condition marked by inconsistencies.
“It's a guide based on clinical circumstances,” Dr. Winter says of the algorithm. “Physicians can deviate when needed, but generally the algorithm brings standardization to our practice and ensures we treat patients in a uniform manner.”
Standardization ensures patients “don't get lost in follow-up,” Dr. Winter says. It also ensures patients don't get overtreated with either unnecessary surgery or MRIs.
The algorithm operates like a flow chart. At the top, it asks whether a patient is a surgical candidate. To determine the answer to that question, the algorithm walks doctors through a series of potential symptoms and treatment options.
After proceeding through the steps, the algorithm suggests one of the following for the patient:
- Surgery
- If the cyst is less than 2 cm, an MRI at six months and then annually until they're no longer a surgical candidate
- If the cyst is greater than or equal to 2 cm, MRIs every six months for one year, then once annually until they're no longer a surgical candidate
RISK OF PANCREATIC CYSTS
Pancreatic cysts are saclike pockets of fluid on the pancreas. Serous cysts are filled with thin fluid and are usually benign. Some subtypes of mucinous cysts, which are filled with a thicker fluid, are more concerning.
 Pictured: a 56-year-old man who had a whipple for an intraductal papillary mucinous tumor with a solid nodule. He went home five days after the whipple with no complications.
Pictured: a 56-year-old man who had a whipple for an intraductal papillary mucinous tumor with a solid nodule. He went home five days after the whipple with no complications.According to the UH algorithm, healthy patients with a long life expectancy (in light of an estimated 8 percent risk of pancreatic cancer at 10 years in cysts that are around 1.5 cm in size) are strong candidates for surgery. “We don't want to perform unnecessary surgery, but we don't want to leave in a potentially cancerous cyst,” Dr. Winter says.
Open surgery has a high rate of complication. The main complications include delayed gastric emptying, pancreatic fistulas and bleeding.1
If the cyst is on the left side, doctors may remove the cyst using minimally invasive surgery. In medium-risk cases, doctors may remove a smaller portion of the pancreas. Other strategies, such as ablading the cyst, are in development, Dr. Winter says.
Because the probability of a cyst developing into cancer remains low, surveillance is a doctor's best tool. The probability that a cyst harbors malignancy at the time of imaging is 0.25 percent, with the overall conversion rate to invasive cancer being 0.24 percent per year, according to an ACG analysis of the SEER database.2 However, retrospective studies of surgically removed cysts put the cancer rate at about 15 percent.
UH TO LAUNCH PANCREATIC CYST CLINIC
The pancreatic cyst algorithm will play an important role in the new UH Pancreatic Cyst Clinic, which launches in May 2019. The team at the Cyst Clinic will evaluate patients with diagnosed or suspected pancreatic cysts.
“Once a week, we can follow and help guide reliable surveillance of pancreatic cysts,” Dr. Winter says. “We may follow some patients remotely through telemedicine or invite them into the clinic. Both physical and virtual visits make it easier for patients to manage this condition.”
Both the clinic and the algorithm are an example of process innovation — not as attention-grabbing as technical innovation, but an important step to improving efficiency and optimizing care. “Although the algorithm is specific to pancreatic cysts, it can serve as a model for standardizing care for complex clinical scenarios,” Dr. Winter says.
To refer a patient for pancreatic cyst evaluation, call 216-844-7874.
REFERENCES
- Scheiman JM, Hwang JH, Moayyedi P. "American gastroenterological association technical review on the diagnosis and management of asymptomatic neoplastic pancreatic cysts." Gastroenterology 2015;148:824–48.
- Lermite, E. et al. "Complications after pancreatic resection: diagnosis, prevention and treatment." Clin Res Hepatol Gastroenterol. 2013 Jun;37(3):230-9. doi: 10.1016/j.clinre.2013.01.003. Epub 2013 Feb 14.