


Multidisciplinary Team Publishes Machine Learning Model for Screening Sleep Disordered Breathing
March 31, 2026
Innovatons in Pulmonology, Critical Care & Sleep Medicine | Spring 2026
University Hospitals Cleveland Medical Center pulmonologist and sleep medicine physician Zachary Strumpf, MD, is the lead author of Spectral analysis of ECG and SpO₂ for machine learning classification of Sleep-Disordered breathing, recently published in the international journal Sleep and Breathing. The article details a pilot study of a machine learning model for screening sleep-disordered breathing (SDB) in hospitalized patients.
 Zachary Strumpf, MD
Zachary Strumpf, MDThe project is a collaboration between faculty members in the University Hospitals Division of Pulmonary, Critical Care and Sleep Medicine and the Case Western Reserve University School of Engineering, including:
- Farhad Kaffashi, Research Assistant Professor, Department of Electrical, Computer and Systems Engineering, School of Engineering
- Kenneth Loparo, PhD, Professor Emeritus, Department of Electrical, Computer, and Systems Engineering, School of Engineering
- Susheel Patil, MD, Director of Sleep Medicine at University Hospitals
- Kingman Strohl, MD, Director of the Sleep Medicine Fellowship at University Hospitals
- Frank Jacono, MD, Division Chief of UH Pulmonary, Critical Care and Sleep Medicine
Addressing a Growing Concern
Estimates indicate that moderate-to-severe obstructive sleep apnea (OSA) affects 24 million Americans and is closely associated with adverse health outcomes, including cardiovascular disease, stroke and increased all-cause mortality. In 2025, the American Academy of Sleep Medicine (AASM) released its first clinical practice guideline for OSA management in medically hospitalized adults. Dr. Patil served as a co-author of the guideline.
The four clinical recommendations include:
- Inpatient screening of OSA in high-risk patients as part of an integrated evaluation and management pathway
- Use of PAP therapy in those with moderate to severe sleep apnea who are currently untreated
- Sleep medicine consultation for those with increased risk of sleep apnea or established sleep apnea
- Discharge plans for management of sleep apnea with a goal to minimize loss to follow-up
“The AASM recognized the importance of expanding OSA diagnosis in the inpatient setting,” Dr. Strumpf says. “However, the task force also noted that sleep medicine resources vary across the country. Our goal is to develop a tool that can leverage commonly monitored physiological signals to increase the capacity to diagnose sleep-disordered breathing at scale.”
There is a known association between untreated sleep apnea and adverse in-hospital and discharge outcomes, including longer length of stay and higher rates of intensive care unit readmission or discharge to a subacute facility rather than home.
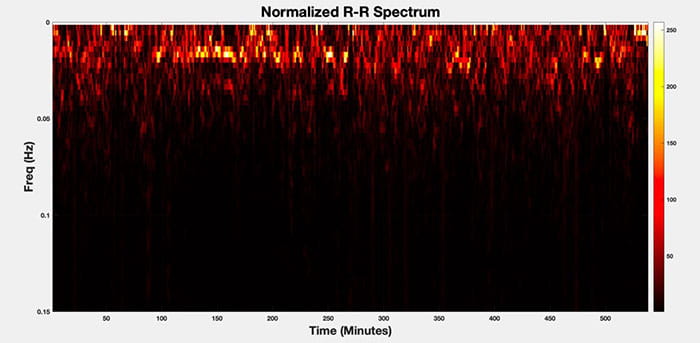 The spectrum of R-R intervals for a sample sleep study.
The spectrum of R-R intervals for a sample sleep study.“When inpatient sleep testing is deferred to outpatient clinics, we miss a potentially treatable diagnosis and an opportunity for improved outcomes,” Dr. Strumpf says. “The first step is to recognize and classify the highest-risk patients so that future work can consolidate and coordinate care pathways that identify those most likely to benefit from early diagnosis and treatment.”
However, Dr. Strumpf explains that testing and diagnosing sleep quality in hospitalized patients remains operationally challenging. It is difficult to determine the optimal timing for testing and to integrate testing equipment and technical expertise into patients’ ongoing hospital care.
Instead of requiring the resources of a comprehensive sleep lab, the team’s algorithm analyzes physiological data routinely collected in the ICU, including electrocardiogram and oxygen saturation. The machine learning tool is paving the way for “smart” monitors that can provide a scalable, non-invasive way to alert providers to breathing issues while the patient is still hospitalized.
“The purpose of the model is to utilize what we call limited-channel analysis of commonly collected physiological signals for the diagnosis of sleep-disordered breathing,” Dr. Strumpf says. “Sleep-disordered breathing and obstructive sleep apnea are incredibly common in the general public and even more common in the inpatient setting.”
The team trained their machine learning model using publicly available data from the Multi-Ethnic Study of Atherosclerosis Sleep cohort, randomly selecting 122 participants, enriched for severe OSA, to train and validate the model to identify SDB.
“This pilot study demonstrated the feasibility of our approach, and the next step is to expand optimization and validation of our model to our University Hospitals ICUs and other inpatient care settings,” Dr. Strumpf says. “Our ongoing research focuses on continuing to validate passive data collection as a tool for screening and risk stratification of sleep-disordered breathing, which will require simultaneous sleep testing and recording inpatient biosignals to iteratively optimize the machine learning model.”